

| << Chapter < Page | Chapter >> Page > |

Visit this site to view the NIH Guide for the Care and Use of Laboratory Animals.
In addition to antibodies against bacteria and viruses to which they have previously been exposed, most individuals also carry antibodies against blood types other than their own. There are presently 33 immunologically important blood-type systems, many of which are restricted within various ethnic groups or rarely result in the production of antibodies. The most important and perhaps best known are the ABO and Rh blood groups (see [link] ).
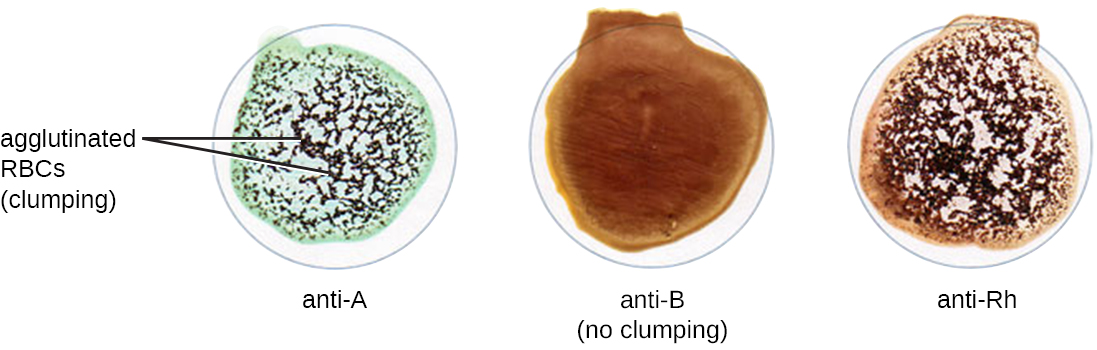
When units of blood are being considered for transfusion , pretransfusion blood testing must be performed. For the blood unit, commercially prepared antibodies against the A, B, and Rh antigens are mixed with red blood cells from the units to initially confirm that the blood type on the unit is accurate. Once a unit of blood has been requested for transfusion, it is vitally important to make sure the donor (unit of blood) and recipient (patient) are compatible for these crucial antigens. In addition to confirming the blood type of the unit, the patient’s blood type is also confirmed using the same commercially prepared antibodies to A, B, and Rh. For example, as shown in [link] , if the donor blood is A-positive, it will agglutinate with the anti-A antiserum and with the anti-Rh antiserum. If no agglutination is observed with any of the sera, then the blood type would be O-negative.
Following determination of the blood type, immediately prior to releasing the blood for transfusion, a cross-match is performed in which a small aliquot of the donor red blood cells are mixed with serum from the patient awaiting transfusion. If the patient does have antibodies against the donor red blood cells, hemagglutination will occur. To confirm any negative test results and check for sensitized red blood cells, Coombs’ reagent may be added to the mix to facilitate visualization of the antibody-red blood cell interaction.
Under some circumstances, a minor cross-match may be performed as well. In this assay, a small aliquot of donor serum is mixed with patient red blood cells. This allows the detection of agglutinizing antibodies in the donor serum. This test is rarely necessary because transfusions generally use packed red blood cells with most of the plasma removed by centrifugation.
Red blood cells have many other antigens in addition to ABO and Rh. While most people are unlikely to have antibodies against these antigens, women who have had multiple pregnancies or patients who have had multiple transfusions may have them because of repeated exposure. For this reason, an antibody screen test is used to determine if such antibodies are present. Patient serum is checked against commercially prepared, pooled, type O red blood cells that express these antigens. If agglutination occurs, the antigen to which the patient is responding must be identified and determined not to be present in the donor unit.
Notification Switch
Would you like to follow the 'Microbiology' conversation and receive update notifications?

|
|

|
|

|
|

|
|

|
|

|
|

|
|
|
|
|

|
|

|